Overview
Adults with an acquired flatfoot deformity may present not with foot deformity but almost uniformly with medial foot pain and decreased function of the affected foot (for a list of causes of an acquired flatfoot deformity in adults. Patients whose acquired flatfoot is associated with a more generalised medical problem tend to receive their diagnosis and are referred appropriately. However, in patients whose adult acquired flatfoot deformity is a result of damage to the structures supporting the medial longitudinal arch, the diagnosis is often not made early. These patients are often otherwise healthier and tend to be relatively more affected by the loss of function resulting from an acquired flatfoot deformity. The most common cause of an acquired flatfoot deformity in an otherwise healthy adult is dysfunction of the tibialis posterior tendon, and this review provides an outline to its diagnosis and treatment.
Causes
As the name suggests, adult-acquired flatfoot occurs once musculoskeletal maturity is reached, and it can present for a number of reasons, though one stands out among the others. While fractures, dislocations, tendon lacerations, and other such traumatic events do contribute to adult-acquired flatfoot as a significant lower extremity disorder, as mentioned above, damage to the posterior tibial tendon is most often at the heart of adult-acquired flatfoot. One study further elaborates on the matter by concluding that ?60% of patients [presenting with posterior tibial tendon damage and adult-acquired flatfoot] were obese or had diabetes mellitus, hypertension, previous surgery or trauma to the medial foot, or treatment with steroids?.
Symptoms
In many cases, adult flatfoot causes no pain or problems. In others, pain may be severe. Many people experience aching pain in the heel and arch and swelling along the inner side of the foot.
Diagnosis
Starting from the knee down, check for any bowing of the tibia. A tibial varum will cause increased medial stress on the foot and ankle. This is essential to consider in surgical planning. Check the gastrocnemius muscle and Achilles complex via a straight and bent knee check for equinus. If the range of motion improves to at least neutral with bent knee testing of the Achilles complex, one may consider a gastrocnemius recession. If the Achilles complex is still tight with bent knee testing, an Achilles lengthening may be necessary. Check the posterior tibial muscle along its entire course. Palpate the muscle and observe the tendon for strength with a plantarflexion and inversion stress test. Check the flexor muscles for strength in order to see if an adequate transfer tendon is available. Check the anterior tibial tendon for size and strength.
Non surgical Treatment
Although AAF is not reversible without surgery, appropriate treatment should address the patient?s current symptoms, attempt to reduce pain, and allow continued ambulation. In the early stages, orthotic and pedorthic solutions can address the loss of integrity of the foot?s support structures, potentially inhibiting further destruction.3-5 As a general principle, orthotic devices should only block or limit painful or destructive motion without reducing or restricting normal motion or muscle function. Consequently, the treatment must match the stage of the deformity.

Surgical Treatment
In cases of PTTD that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required. For some advanced cases, surgery may be the only option. Your foot and ankle surgeon will determine the best approach for you.
Adults with an acquired flatfoot deformity may present not with foot deformity but almost uniformly with medial foot pain and decreased function of the affected foot (for a list of causes of an acquired flatfoot deformity in adults. Patients whose acquired flatfoot is associated with a more generalised medical problem tend to receive their diagnosis and are referred appropriately. However, in patients whose adult acquired flatfoot deformity is a result of damage to the structures supporting the medial longitudinal arch, the diagnosis is often not made early. These patients are often otherwise healthier and tend to be relatively more affected by the loss of function resulting from an acquired flatfoot deformity. The most common cause of an acquired flatfoot deformity in an otherwise healthy adult is dysfunction of the tibialis posterior tendon, and this review provides an outline to its diagnosis and treatment.
Causes
As the name suggests, adult-acquired flatfoot occurs once musculoskeletal maturity is reached, and it can present for a number of reasons, though one stands out among the others. While fractures, dislocations, tendon lacerations, and other such traumatic events do contribute to adult-acquired flatfoot as a significant lower extremity disorder, as mentioned above, damage to the posterior tibial tendon is most often at the heart of adult-acquired flatfoot. One study further elaborates on the matter by concluding that ?60% of patients [presenting with posterior tibial tendon damage and adult-acquired flatfoot] were obese or had diabetes mellitus, hypertension, previous surgery or trauma to the medial foot, or treatment with steroids?.
Symptoms
In many cases, adult flatfoot causes no pain or problems. In others, pain may be severe. Many people experience aching pain in the heel and arch and swelling along the inner side of the foot.
Diagnosis
Starting from the knee down, check for any bowing of the tibia. A tibial varum will cause increased medial stress on the foot and ankle. This is essential to consider in surgical planning. Check the gastrocnemius muscle and Achilles complex via a straight and bent knee check for equinus. If the range of motion improves to at least neutral with bent knee testing of the Achilles complex, one may consider a gastrocnemius recession. If the Achilles complex is still tight with bent knee testing, an Achilles lengthening may be necessary. Check the posterior tibial muscle along its entire course. Palpate the muscle and observe the tendon for strength with a plantarflexion and inversion stress test. Check the flexor muscles for strength in order to see if an adequate transfer tendon is available. Check the anterior tibial tendon for size and strength.
Non surgical Treatment
Although AAF is not reversible without surgery, appropriate treatment should address the patient?s current symptoms, attempt to reduce pain, and allow continued ambulation. In the early stages, orthotic and pedorthic solutions can address the loss of integrity of the foot?s support structures, potentially inhibiting further destruction.3-5 As a general principle, orthotic devices should only block or limit painful or destructive motion without reducing or restricting normal motion or muscle function. Consequently, the treatment must match the stage of the deformity.
Surgical Treatment
In cases of PTTD that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required. For some advanced cases, surgery may be the only option. Your foot and ankle surgeon will determine the best approach for you.
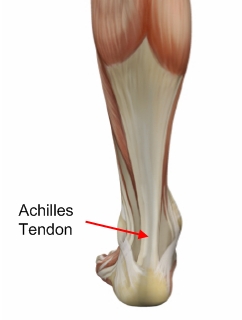 Inflammation of the Achilles tendon.The Achilles is the large tendon connecting the two major calf muscles, gastrocnemius and soleus, to the back of the heel bone. Under too much stress, the tendon tightens and is forced to work too hard. This causes it to become inflamed (that is tendinitis), and, over time, can produce a covering of scar tissue, which is less flexible than the tendon. If the inflamed Achilles continues to be stressed, it can tear or rupture.
Inflammation of the Achilles tendon.The Achilles is the large tendon connecting the two major calf muscles, gastrocnemius and soleus, to the back of the heel bone. Under too much stress, the tendon tightens and is forced to work too hard. This causes it to become inflamed (that is tendinitis), and, over time, can produce a covering of scar tissue, which is less flexible than the tendon. If the inflamed Achilles continues to be stressed, it can tear or rupture.

 RSS Feed
RSS Feed
